PERRLA meaning refers to a standard shorthand clinicians write after checking your eyes during a physical or neurological exam: Pupils Equal, Round, Reactive to Light and Accommodation. When a chart says PERRLA, it means both pupils looked the same size, had a normal round shape, and responded normally when a light was shone into them and when focusing on a near object. This guide explains what each letter checks for, how the exam is performed, what an abnormal finding can suggest, and what to know if your own notes mention PERRLA or a pupil abnormality.
What PERRLA stands for and means on a chart
PERRLA is an acronym clinicians use in physical exam notes, most often under a “HEENT” (head, eyes, ears, nose, throat) or neurological section. Each letter documents one part of a quick pupil check:
- P — Pupils
- E — Equal (both pupils are the same size)
- R — Round (both pupils have a regular, circular shape)
- R — Reactive (pupils constrict appropriately)
- L — to Light (the reaction happens when a light is shone into the eye)
- A — and Accommodation (the reaction happens when focusing on a near object)
Seeing PERRLA in a note is a shorthand way of saying “the pupil exam was normal at this visit.” It does not describe a lab value or a diagnosis; it is an observation from a bedside or in-office exam, similar in spirit to related shorthand like documenting that a patient shows no acute distress or noting normal findings elsewhere in a physical exam.
How the pupillary exam is performed
Clinicians typically check pupils in a dimly lit room so the pupils are naturally semi-dilated, which makes changes easier to see. The exam usually has two parts.
The light reaction (direct and consensual response)
The examiner shines a penlight into one eye and watches that pupil constrict (the direct response), then checks whether the other pupil also constricts even though no light was shone into it (the consensual response). This happens because the nerve signal from one eye normally reaches the pupil-control centers for both eyes.
The swinging-light test
To look for subtler problems, clinicians often move the light back and forth between the two eyes every few seconds, a technique called the swinging-light test. In a healthy pupillary reflex, each eye should constrict at roughly the same speed and to a similar degree as the light swings over. If one eye appears to dilate instead of constrict when the light swings onto it, this can point to a problem with that eye’s optic nerve, a finding sometimes called a relative afferent pupillary defect.
The accommodation (near) response
The examiner then asks the patient to focus on a distant object and then switch focus to something held close, such as a finger a few inches from the nose. Normally, both pupils constrict slightly as the eyes converge and focus up close. This near response is what the “A” in PERRLA documents.
What each letter of PERRLA checks for
Breaking down the exam helps explain why clinicians look at more than just whether the pupils react.
Equal size (anisocoria check)
Clinicians compare pupil size between the two eyes. A difference in pupil size between eyes is called anisocoria. A small, stable difference can be a lifelong, harmless trait in some people, but a new or changing difference deserves prompt attention because it can signal a problem affecting the nerves or muscles that control the pupil.
Round shape
A normal pupil is a smooth circle. An irregular or oval shape can result from prior eye surgery, trauma, inflammation inside the eye, or certain neurological conditions, so clinicians note shape along with size.
Reactive to light and accommodation
The reactive component checks that the pupil constricts briskly and to a similar extent on both sides. Clinicians typically grade the briskness of the reaction and note whether it is symmetric between the two eyes.
What an abnormal pupil finding can suggest
When pupils are not equal, round, and reactive, clinicians describe the specific abnormality rather than writing PERRLA. Common examples include a pupil that reacts slowly or not at all, a pupil that is much larger or smaller than its partner, or one that fails to constrict during the swinging-light test. According to a widely referenced clinical examination text published through the National Institutes of Health’s NCBI Bookshelf, the pupil is considered abnormal if it fails to dilate in the dark or fails to constrict to light or accommodation, and unequal pupil size unrelated to local eye disease should not be attributed simply to lighting or eye anatomy (NCBI Bookshelf: The Pupils).
Possible causes of abnormal pupil findings range from benign to urgent. Some people have a lifelong, stable difference in pupil size that never changes and causes no other symptoms. Others develop sudden anisocoria or a sluggish pupil because of nerve compression, medication effects, eye drops, prior eye surgery, or, less commonly, a problem inside the skull affecting the nerves that control the pupil.
Why PERRLA is part of routine neuro, eye, and trauma exams
Pupil checks are quick, require no special equipment beyond a penlight, and provide information about how well the eyes, optic nerves, and the parts of the brainstem that control pupil size are working together. Because of this, PERRLA or a pupil assessment appears in several different contexts:
- Routine physical exams, alongside other baseline checks such as an orientation assessment of alertness and awareness.
- Eye exams, where pupil size and reaction are checked alongside other structures, sometimes documented using related shorthand for the right eye, the left eye, or both eyes together.
- Neurological exams, often paired with other quick checks such as deep tendon reflex testing to build a fuller picture of nervous system function.
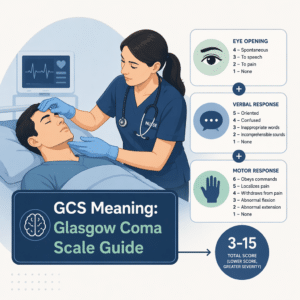
- Emergency and trauma evaluations, where pupil findings are recorded alongside a level-of-consciousness score such as the Glasgow Coma Scale, because pupil changes can appear before or alongside changes in alertness.
In critical care and trauma settings specifically, pupil findings carry extra weight. The Centers for Disease Control and Prevention’s clinical guideline checklist for pediatric mild traumatic brain injury directs clinicians to examine for findings that suggest a more serious injury, explicitly naming pupillary asymmetry as one such warning sign to check for during the physical exam (CDC: Safety Guidelines for Pediatric Mild TBI). Similarly, the National Institute of Neurological Disorders and Stroke lists unequal eye pupil size or dilation among the physical symptoms that warrant immediate medical attention within the first 24 hours after a head injury (NINDS: Traumatic Brain Injury).
Normal versus abnormal pupil findings
| Finding | What it looks like | Possible significance |
|---|---|---|
| PERRLA (normal) | Pupils equal, round, and briskly reactive to light and near focus on both sides | Expected, healthy finding at that exam |
| Anisocoria | One pupil is visibly larger or smaller than the other | Can be a harmless lifelong trait; new or changing anisocoria warrants prompt evaluation |
| Sluggish or absent light reaction | Pupil constricts slowly, partially, or not at all when light is shone in | May reflect an issue along the nerve pathway that controls the pupil, medication effects, or eye disease |
| Irregular shape | Pupil is oval or notched rather than a smooth circle | Can follow prior eye surgery, trauma, or inflammation inside the eye |
| Failed swinging-light test | One pupil appears to dilate instead of constrict as light swings onto it | Suggests a relative afferent pupillary defect, often linked to an optic nerve issue |
When to seek immediate care
Most of the time, a pupil check is a routine, reassuring part of a visit. However, certain pupil changes are considered warning signs, particularly after a head injury or when they appear suddenly. Seek emergency care right away if you or someone you are with develops any of the following, especially within 24 hours of a blow to the head:
- Pupils that are suddenly unequal in size when they were not before.
- A pupil that stops reacting to light on one or both sides.
- Unequal pupils together with a severe or worsening headache, repeated vomiting, slurred speech, new weakness, seizures, or increasing difficulty staying awake.
- Any new pupil change following a car accident, a fall, a sports collision, or another impact to the head.
These combinations of symptoms are exactly the kind of findings that the CDC’s pediatric mild TBI checklist and the NINDS guidance flag as reasons for urgent evaluation, since they can point to bleeding or swelling inside the skull that needs prompt treatment.
What patients should know if their chart notes PERRLA or an abnormality
If your chart or discharge notes say PERRLA, that is a reassuring, normal finding from that specific exam. It does not mean every possible eye or brain condition has been ruled out; it means the pupil portion of the exam looked healthy at that moment. If instead your notes mention anisocoria, a sluggish pupil, or another abnormality, it is reasonable to ask your clinician what the finding means, whether it is new or previously known, and whether any follow-up testing is planned. Bringing old photographs can sometimes help a clinician determine whether a pupil difference is truly new or has simply gone unnoticed for a long time.
Latest scientific advances
Recent research has focused on how reliable the traditional, penlight-based pupil exam really is, and whether newer tools can do better. A 2022 study published in PLoS ONE compared manual pupil measurements against an automated, camera-based pupil-measuring device (called a pupillometer) in critically ill patients. The manual exam agreed reasonably well between two examiners, but the device was roughly twice as consistent and repeatable, and the study found that examiners missed about one in four abnormal pupil reactions that the device picked up. In plain terms, this suggests the classic bedside pupil check is useful but has real limits when it comes to catching subtle changes, especially in patients who are critically ill.
Building on this, a large multicenter study called ORANGE, published in The Lancet Neurology in 2023, followed more than 500 patients with serious brain injuries (including traumatic brain injury, bleeding around the brain, and bleeding within the brain) using a device-based pupil reactivity score. The study found that a lower pupil reactivity score was linked to a meaningfully higher chance of poor long-term recovery and death, supporting the idea that closely tracking pupil reactivity over time, not just checking it once, helps clinicians monitor how a serious brain injury is evolving.
A 2024 narrative review in the Journal of Clinical Medicine summarized how these automated, camera-based pupil devices are increasingly used alongside the traditional penlight exam in intensive care, particularly for patients with traumatic brain injury. The review noted that while these devices are valuable for detecting subtle changes and supporting monitoring over time, they are intended to complement, not replace, careful clinical examination and other forms of monitoring such as imaging.
Together, these findings help explain why a classic acronym like PERRLA remains useful for everyday, low-risk situations, while more detailed or repeated pupil measurements, sometimes using specialized devices, are increasingly used in intensive care and neuro-critical settings where subtle changes matter most.
Glossary
| Term | Definition |
|---|---|
| Anisocoria | A difference in size between the two pupils. It can be a harmless, lifelong trait or a sign of a new problem, depending on whether it is longstanding or newly noticed. |
| Accommodation | The eye’s process of adjusting focus from a distant object to a near one, which normally causes both pupils to constrict slightly. |
| Pupillary light reflex | The automatic narrowing of the pupil in response to light shone into the eye, and the corresponding widening in dim light. |
| Swinging-light test | An exam technique where a light is moved back and forth between the two eyes to compare how briskly each pupil reacts. |
| Relative afferent pupillary defect | A finding, sometimes called a Marcus Gunn sign, where one pupil appears to dilate instead of constrict during the swinging-light test, often pointing to an optic nerve problem on that side. |
| Pupillometer | A handheld, camera-based device that measures pupil size and reaction speed more precisely and consistently than a visual exam alone. |
| Neurological exam | A structured physical exam that checks nerve and brain function, including alertness, movement, sensation, reflexes, and pupil responses. |
| Traumatic brain injury (TBI) | An injury to the brain caused by an outside force, such as a blow, jolt, or penetrating injury, ranging from mild to severe. |
FAQ
Q: What does PERRLA stand for exactly?
A: PERRLA stands for Pupils Equal, Round, and Reactive to Light and Accommodation. It is shorthand clinicians write after a normal pupil exam, meaning both pupils were the same size, had a regular round shape, and constricted appropriately both to light and when focusing on a near object.
Q: Is PERRLA always checked together with EOMI?
A: PERRLA is often documented alongside EOMI, which stands for extraocular movements intact and refers to a separate check that the eyes move normally in all directions. Together, PERRLA and EOMI give a quick snapshot of pupil function and eye movement during a routine or neurological exam, though they assess different aspects of eye health.
Q: Does a normal PERRLA finding rule out a brain injury?
A: No. A normal PERRLA finding means the pupil portion of the exam looked healthy at that specific moment, but it is only one part of a broader evaluation. Clinicians combine pupil findings with a person’s symptoms, level of alertness, and, when needed, imaging to assess for a brain injury.
Q: Why do some people naturally have unequal pupils?
A: About one in five healthy people have a lifelong, stable difference in pupil size known as essential or physiologic anisocoria. This type of difference stays roughly the same regardless of lighting and does not change over time, which helps distinguish it from a newly developed problem.
Q: How is the pupil exam different from an automated pupillometer reading?
A: The traditional exam uses a handheld penlight and the clinician’s visual judgment to grade how a pupil reacts. An automated pupillometer instead uses a small camera to measure pupil size and reaction speed numerically, which can pick up on subtle changes that may be harder to detect by eye alone, particularly in critically ill patients.
Q: What should I do if my chart shows an abnormal pupil finding instead of PERRLA?
A: Ask your clinician what the specific finding means, whether it is a new change or something previously documented, and whether any follow-up is recommended. If the finding developed suddenly or came with other symptoms such as a severe headache or confusion, treat it as a reason to seek prompt medical attention.
Sources
- Spector RH — The Pupils, in Clinical Methods: The History, Physical, and Laboratory Examinations, 3rd edition — NCBI Bookshelf, National Library of Medicine, National Institutes of Health, 1990 (chapter last referenced 2026). https://www.ncbi.nlm.nih.gov/books/NBK381/
- Cleveland Clinic — Pupillary Light Reflex (PLR): What It Is and How It Works — Cleveland Clinic Health Library, medically reviewed, 2026. https://my.clevelandclinic.org/health/articles/pupillary-light-reflex-plr
- Centers for Disease Control and Prevention — Safety Guidelines for Pediatric Mild TBI (Pediatric Mild Traumatic Brain Injury Guideline Checklist) — CDC Traumatic Brain Injury & Concussion, 2025. https://www.cdc.gov/traumatic-brain-injury/hcp/clinical-guidance/pediatric-mtbi.html
- National Institute of Neurological Disorders and Stroke — Traumatic Brain Injury (TBI) — NINDS Health Information, National Institutes of Health, 2026. https://www.ninds.nih.gov/health-information/disorders/traumatic-brain-injury-tbi
- Nyholm B, et al. — Superior reproducibility and repeatability in automated quantitative pupillometry compared to standard manual assessment, and quantitative pupillary response parameters present high reliability in critically ill cardiac patients — PLoS ONE, 2022. https://consensus.app/papers/details/7107dd74c6ca5833b82f63d45ef904ac/?utm_source=claude_code
- Oddo M, et al. — The Neurological Pupil index for outcome prognostication in people with acute brain injury (ORANGE): a prospective, observational, multicentre cohort study — The Lancet Neurology, 2023. https://doi.org/10.1016/S1474-4422(23)00271-5
- Vrettou CS, et al. — The Role of Automated Infrared Pupillometry in Traumatic Brain Injury: A Narrative Review — Journal of Clinical Medicine, 2024. https://doi.org/10.3390/jcm13020614
Further reading
- GCS Meaning: Glasgow Coma Scale Guide
- DTR Meaning: Deep Tendon Reflex Guide
- NAD Meaning: No Acute Distress in Notes
- OU Meaning: Both Eyes (Oculus Uterque)
- Neuron-Specific Enolase: Understanding Your Results
Exam findings like PERRLA are a small but meaningful part of a much larger picture of health, one that also includes the lab and imaging results gathered during routine care or after an injury. Understanding your own results, whether that is a basic metabolic panel, a complete blood count, or a specialized marker ordered after a neurological concern, can make follow-up conversations with your care team clearer and more focused. Reviewing these numbers alongside physical exam findings helps connect the dots between how you feel, what a clinician observes, and what your test results actually show, always as a support for understanding rather than a replacement for medical evaluation.